Moyamoya disease
Progressive terminal ICA-centered narrowing with characteristic collateral networks.
Moyamoya disease narrows major arteries at the base of the brain. The brain may form small collateral vessels to route blood around the narrowing, but these routes may not prevent a TIA, stroke, or bleeding. Specialists use several imaging tests to understand the arteries, prior injury, and blood flow before discussing treatment.
Moyamoya disease is a progressive steno-occlusive arteriopathy centered on the terminal intracranial internal carotid arteries and their proximal branches, with characteristic collateral networks. Clinical decisions integrate ischemic or hemorrhagic presentation, vascular anatomy, parenchymal injury, collateral pathways, and hemodynamic reserve.
AI-generated educational schematic. Not a real medical image or an exact anatomical representation.
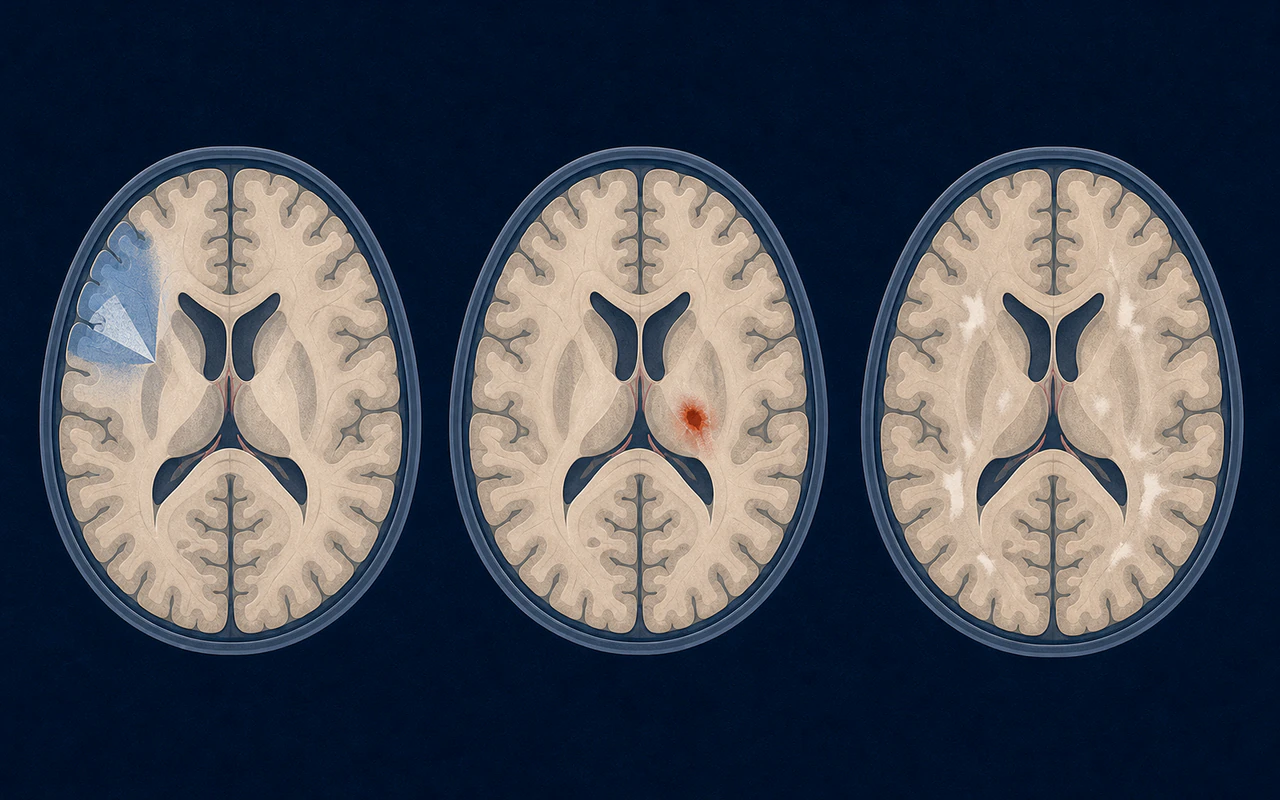
MRI evaluates acute and chronic brain injury and helps assess alternative diagnoses.
AI-generated educational schematic. Not a real medical image or an exact anatomical representation.
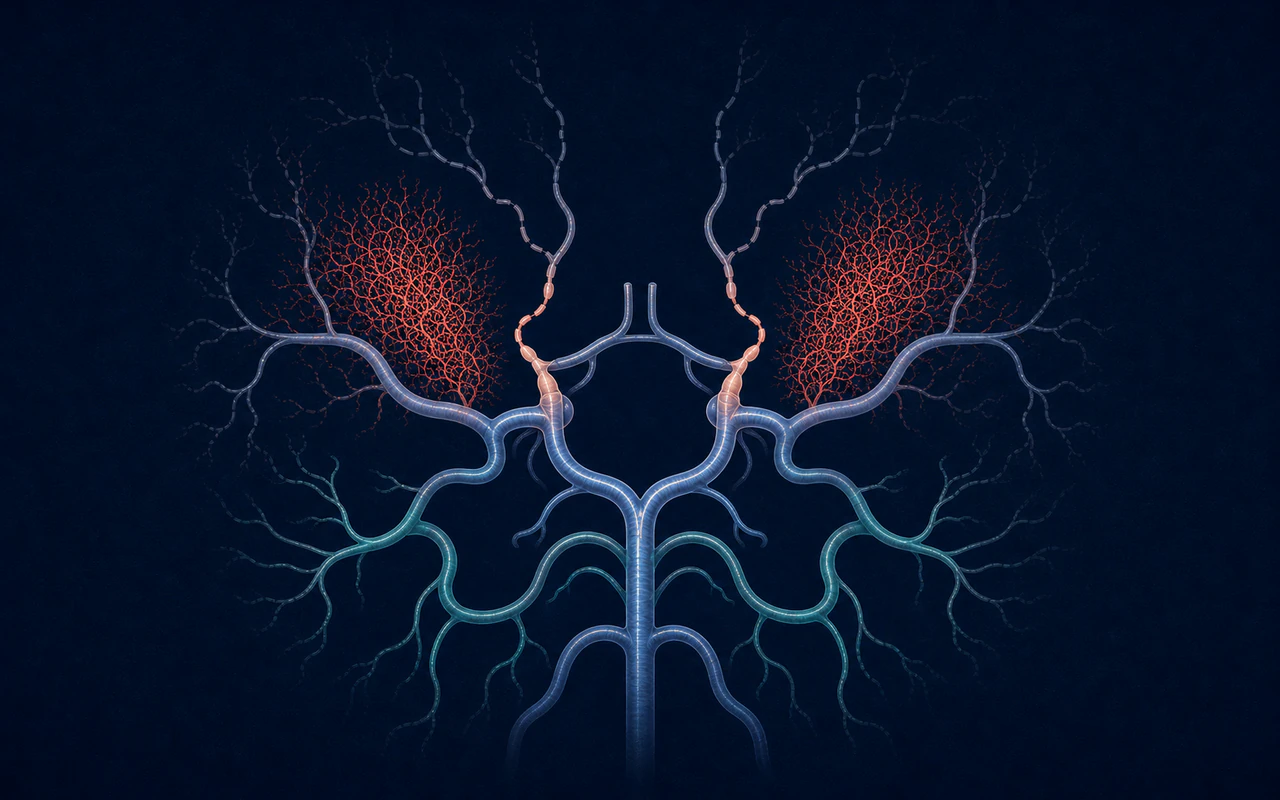
MRA provides a noninvasive view of major intracranial arterial narrowing.
AI-generated educational schematic. Not a real medical image or an exact anatomical representation.
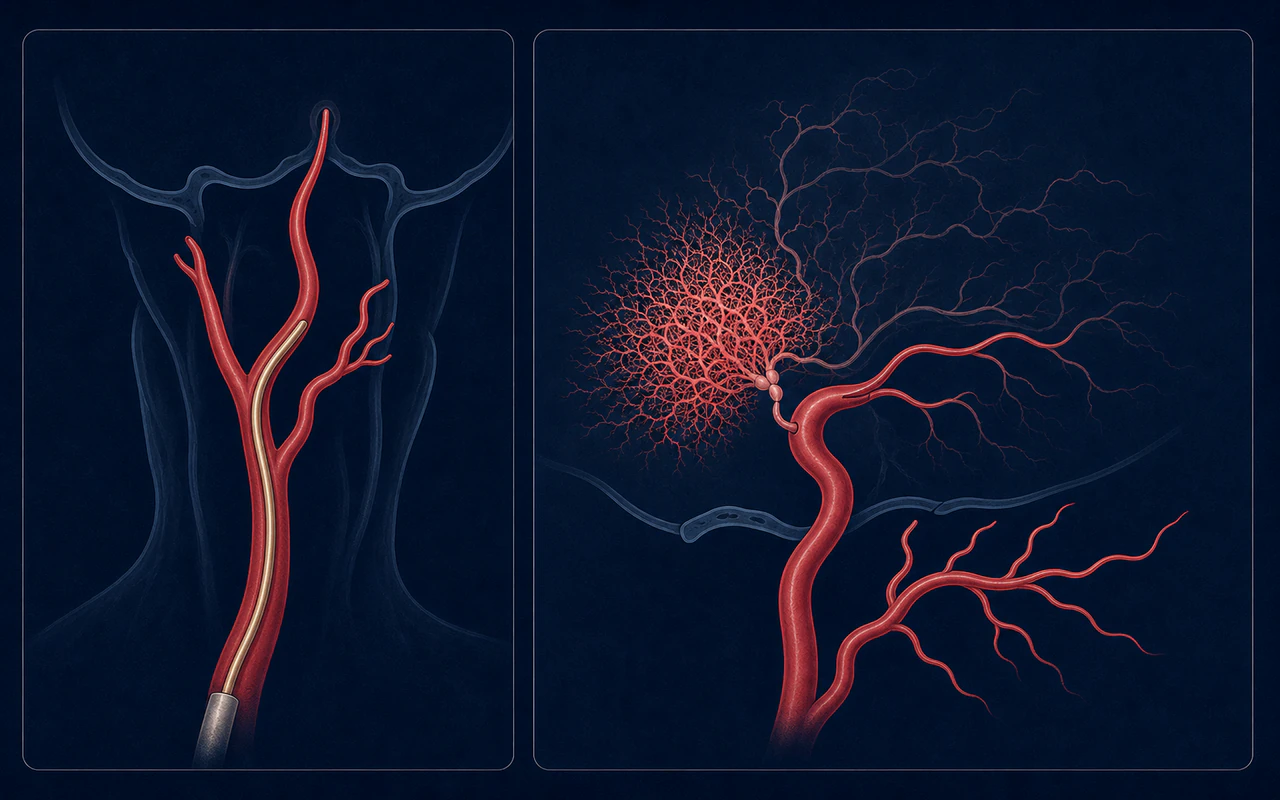
DSA defines stenosis, collateral routes, donor anatomy, and angiographic stage in high detail.
AI-generated educational schematic. Not a real medical image or an exact anatomical representation.
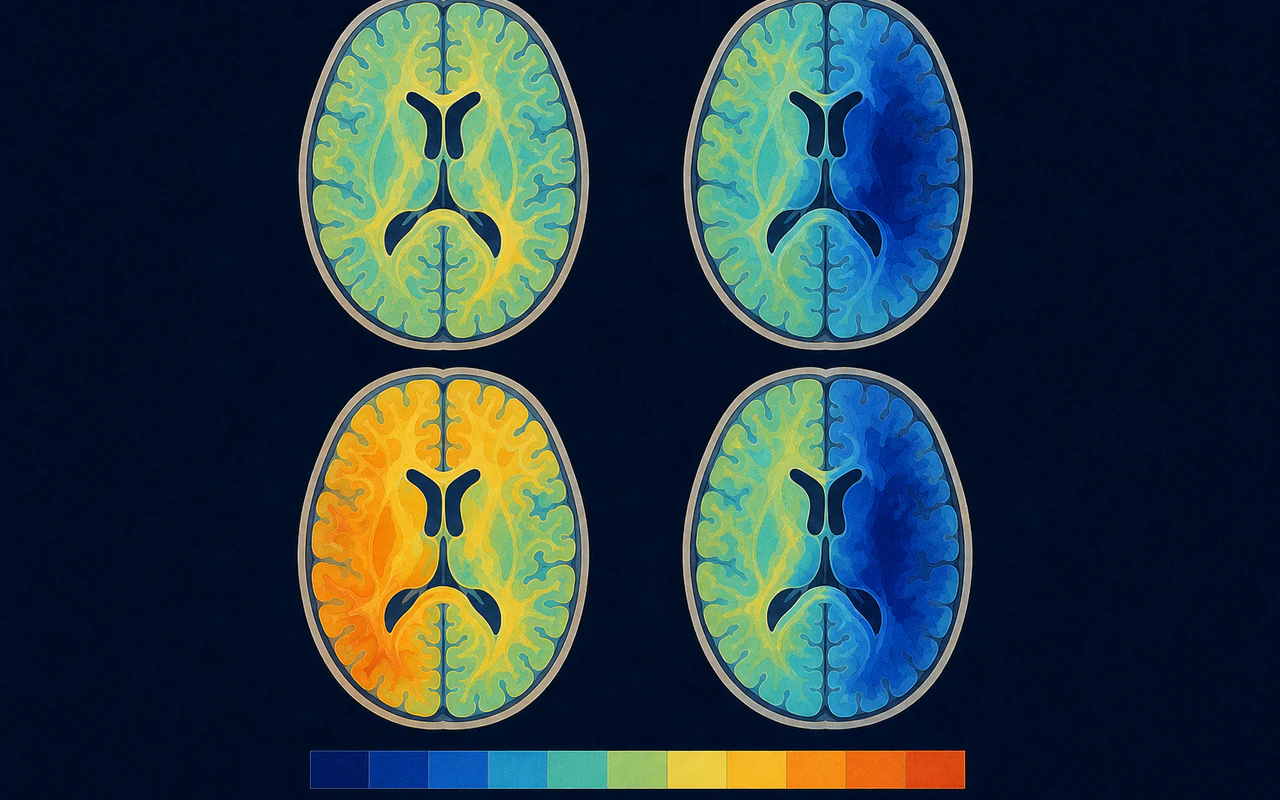
Perfusion and reserve methods assess how effectively tissue is supplied and responds to challenge.
AI-generated educational schematic. Not a real medical image or an exact anatomical representation.
Follow-up imaging may assess direct bypass patency, indirect collateral growth, perfusion, and untreated territories.
Progressive terminal ICA-centered narrowing with characteristic collateral networks.
Plaque-related stenosis interpreted with age, risk factors, vessel wall, and distribution.
Inflammatory arteriopathy assessed with clinical, laboratory, vessel-wall, and distribution clues.
Usually presents with acute headache and reversible multifocal arterial narrowing.
Arterial injury occurs in a prior radiation field and may produce a moyamoya pattern.
Focal arterial wall injury may mimic stenosis but has a different mechanism and course.
Frames adult moyamoya disease and syndrome around presentation, imaging, hemodynamics, and individualized revascularization decisions.
Read registered sourceProvides European consensus on diagnostic workup, referral expertise, medical care, and surgical strategy.
Read registered sourceAddresses ischemic and hemorrhagic presentations, revascularization approaches, and perioperative management.
Read registered sourceIn moyamoya disease, the terminal portions of the internal carotid arteries and nearby branches become narrowed or blocked over time. The brain may respond by forming a network of small collateral vessels. On an angiogram, that network can resemble a “puff of smoke,” which is the origin of the Japanese name moyamoya. The disorder can affect one or both sides and can occur in children or adults. [1]
The diagnosis is based on characteristic vascular findings and a clinical assessment that considers other possible causes. Current diagnostic criteria recognize both unilateral and bilateral disease. When a similar arterial pattern occurs together with another condition, clinicians generally use the term moyamoya syndrome rather than primary moyamoya disease. [2]
Takeuchi and Shimizu reported a case with hypoplasia of the internal carotid arteries in 1957. The descriptive term moyamoya was introduced later, in 1969, so the first report and the naming of the disease are separate historical milestones. [3]
Reduced blood flow can produce transient ischemic attacks, ischemic stroke, headaches, seizures, or changes in cognition. Fragile collateral vessels may also rupture and cause intracranial hemorrhage. Presentation varies with age, vascular territory, and the brain’s ability to maintain blood flow. [4]
Evaluation commonly combines MRI, MRA, digital subtraction angiography, and tests of cerebral perfusion or cerebrovascular reserve. These tests answer different questions: anatomy, prior brain injury, collateral pathways, and whether blood flow can increase when needed.
Treatment is individualized. Medicines may be used for selected symptoms or stroke prevention, but they do not reopen the progressively narrowed arteries. Revascularization surgery creates or encourages new routes for blood to reach the brain and is a central treatment consideration for symptomatic patients or patients with impaired hemodynamics. Decisions should be made by a team experienced with moyamoya because evidence, anatomy, age, and presentation all influence the plan. [5]
Moyamoya is an angiographic and clinical diagnosis, not simply a description of any intracranial stenosis. Atherosclerosis, vasculitis, dissection, radiation injury, and genetic or systemic disorders can produce overlapping findings. Specialist review of the vessel wall, outer arterial diameter, collateral pattern, and associated conditions helps distinguish these entities.