Multiple sclerosis
Typical clinical and paraclinical evidence with characteristic dissemination and no better explanation.
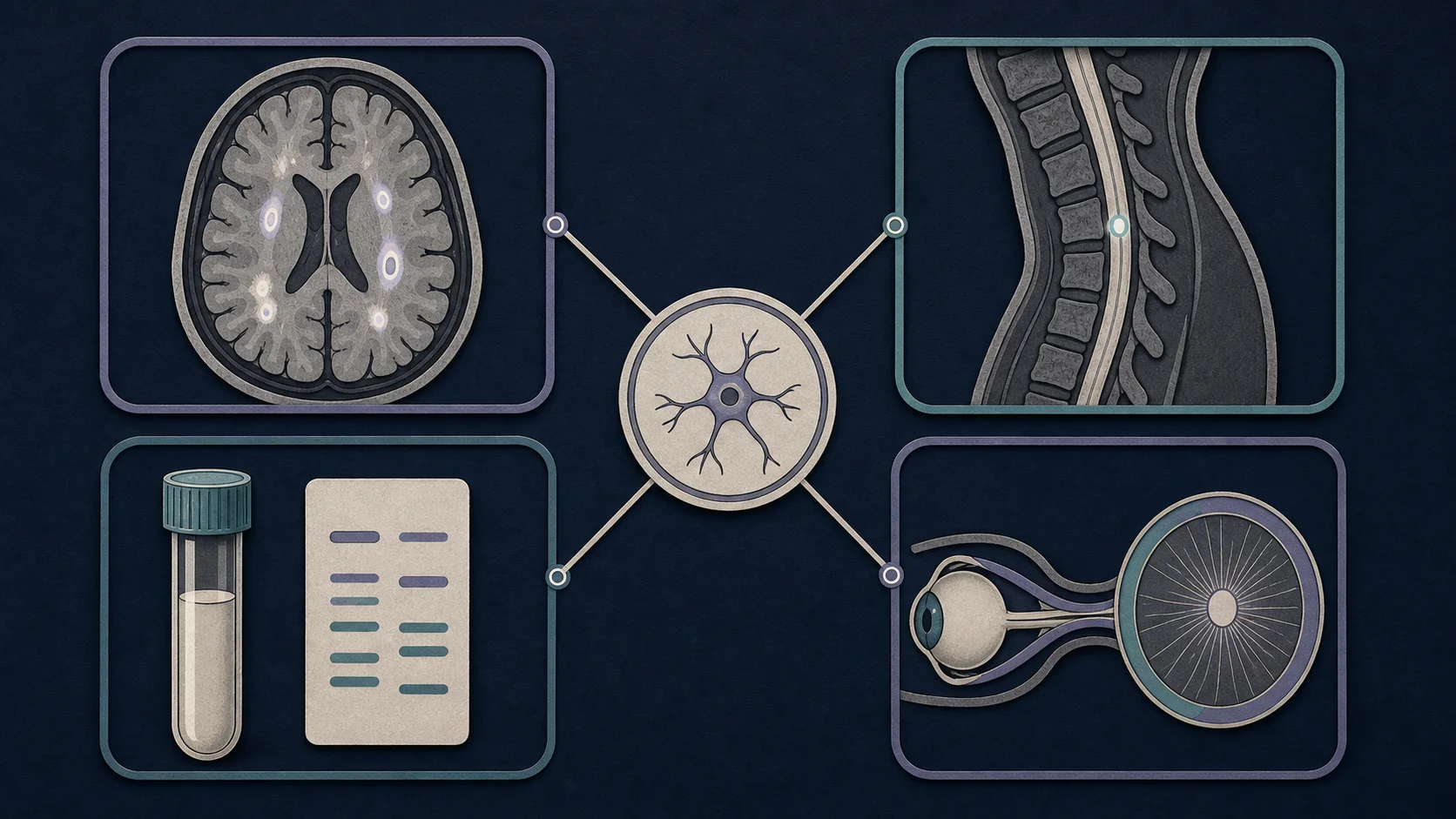
There is no single symptom, scan, or blood test that diagnoses multiple sclerosis by itself. The workup asks whether the history and examination fit a central nervous system demyelinating disorder, whether objective evidence is distributed in a characteristic way, and whether another diagnosis explains the findings better.
Diagnostic synthesis combines a compatible presentation, lesion distribution, temporal evidence, biomarkers, and exclusion of a better explanation. The published McDonald criteria organize that evidence, but correct application still depends on clinical judgment.
AI-generated educational schematic. Not a real medical image or an exact anatomical representation.
Brain MRI assesses lesion location, morphology, enhancement, and interval change.
AI-generated educational schematic. Not a real medical image or an exact anatomical representation.
Spinal imaging can identify cord lesions and evaluate structural alternatives.
AI-generated educational schematic. Not a real medical image or an exact anatomical representation.
CSF can provide evidence of intrathecal immune activity but does not diagnose MS in isolation.
Typical clinical and paraclinical evidence with characteristic dissemination and no better explanation.
Aquaporin-4 antibody-associated disease can require different long-term treatment and must not be mislabeled as MS.
MOG antibody-associated optic neuritis, myelitis, or brain inflammation has overlapping but distinct patterns.
Nonspecific white-matter lesions require interpretation by location, morphology, age, risk factors, and symptoms.
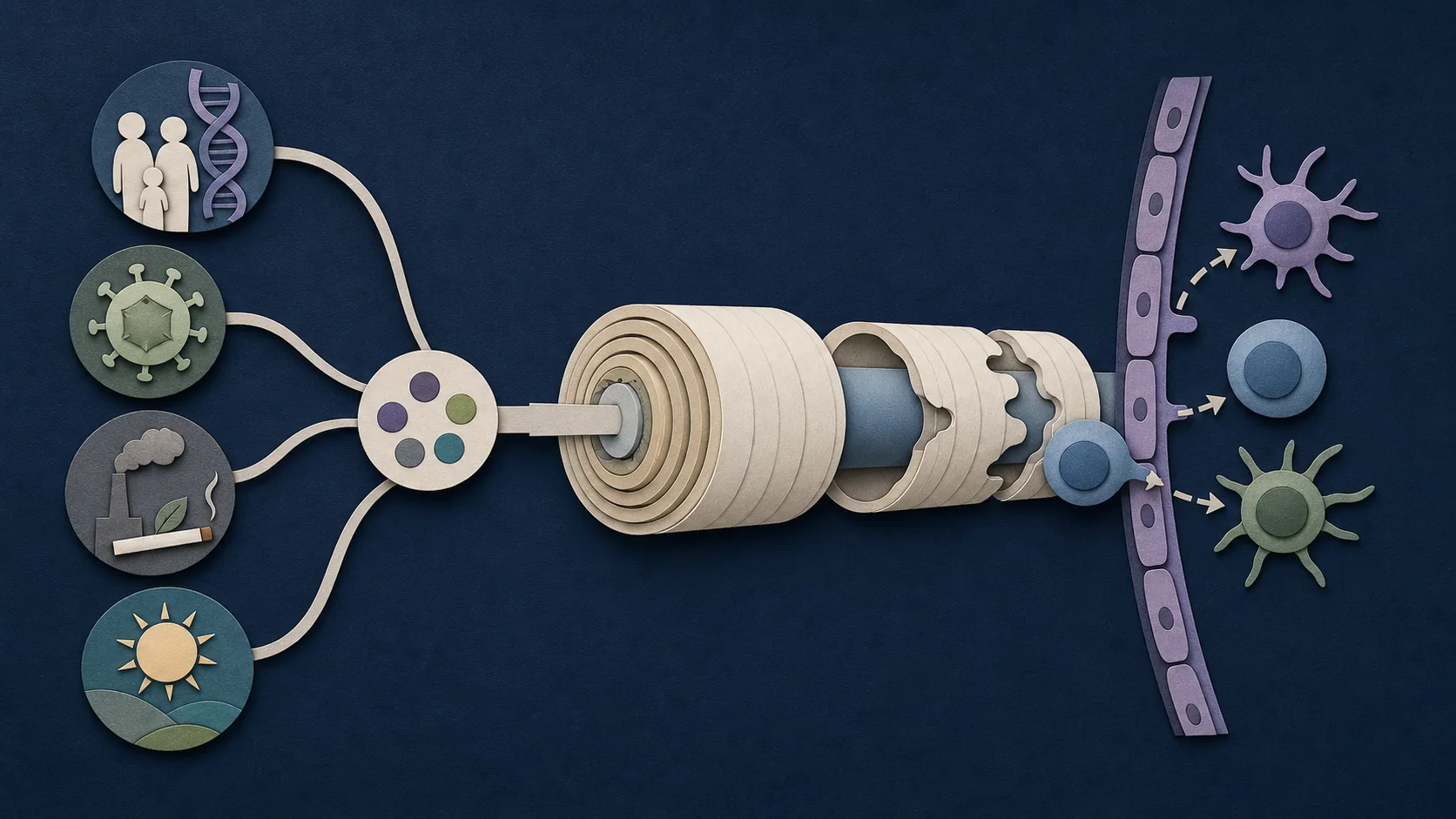
History, examination, blood and CSF studies, imaging, and systemic findings may identify another mechanism.
Compression, deficiency, toxic injury, and inherited disorders can mimic selected clinical or imaging features.
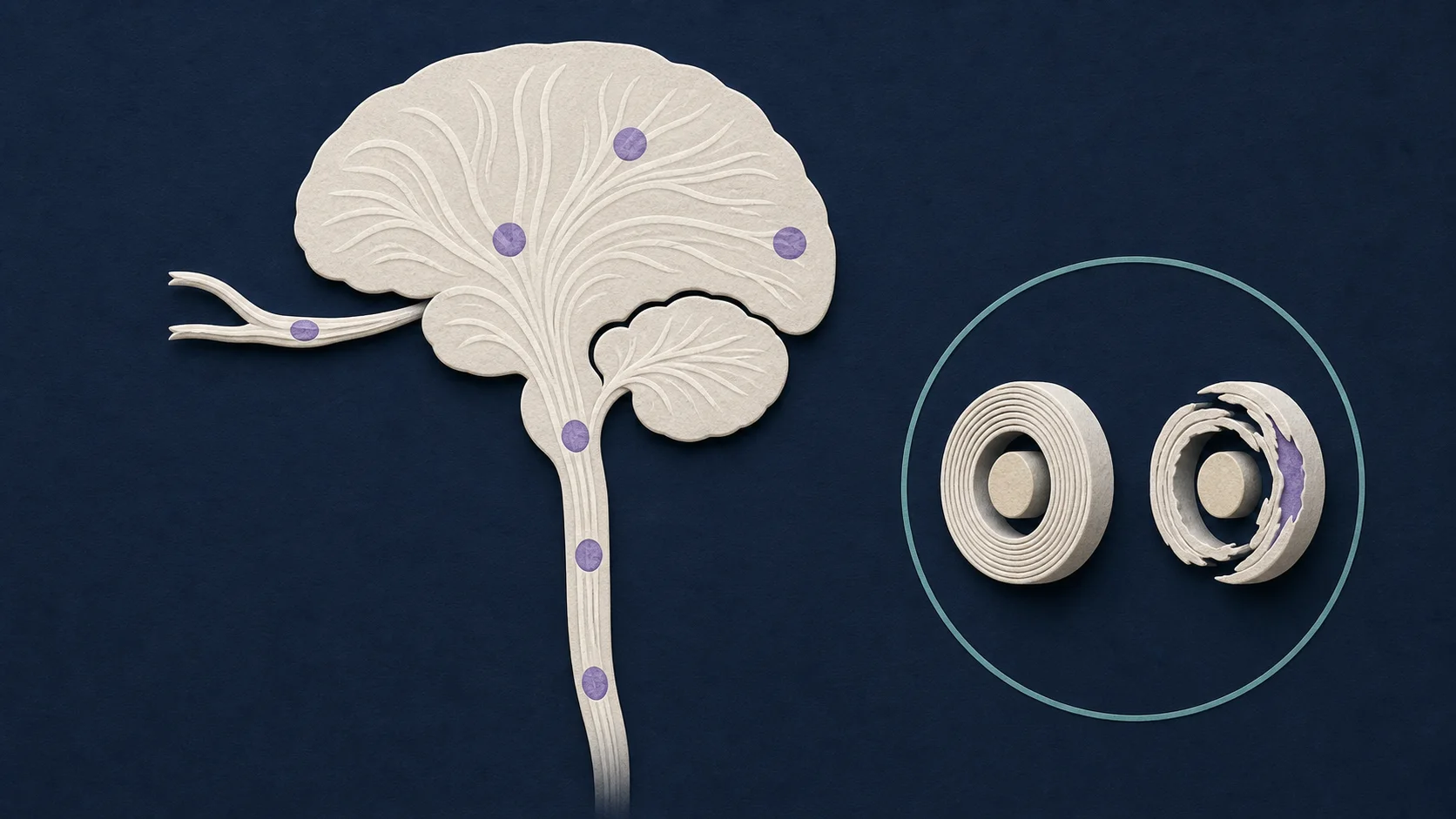
MRI evaluates the brain and, when indicated, the spinal cord and optic nerves. Specialists assess lesion location, morphology, enhancement, and change over time rather than counting all white-matter spots equally. Standardized acquisition improves comparison across visits. [1]
A lumbar puncture may assess CSF-specific oligoclonal bands or kappa free light chains, cell count, protein, and tests for alternative diagnoses. Objective optic nerve evidence may come from MRI, optical coherence tomography, or visual evoked potentials in defined circumstances.
The 2024 criteria include the optic nerve as a fifth central nervous system location and provide roles for CSF and susceptibility-based markers such as the central vein sign and paramagnetic rim lesions. They also address selected people with radiologically isolated findings. These additions do not remove the need for a compatible context and careful exclusion of mimics. [2]
Diagnostic certainty depends on data quality. MRI field strength, sequence, slice thickness, motion, lesion location, prior scans, steroid timing, and gadolinium use can affect interpretation. Atypical symptoms or imaging should increase, not lower, attention to alternative diagnoses.