Multiple sclerosis
A compatible central nervous system syndrome with characteristic dissemination and no better explanation.
Multiple sclerosis affects the brain, spinal cord, and optic nerves. Immune activity damages myelin and can also injure nerve fibers, creating lesions in different parts of the central nervous system. The location and timing of those lesions help explain why symptoms and long-term effects vary so widely.
Multiple sclerosis is a chronic immune-mediated disease of the central nervous system characterized by inflammation, demyelination, neuroaxonal injury, and variable repair. Clinical care distinguishes new inflammatory activity from recovery, accumulated injury, progression, comorbidity, and symptoms caused by another condition.
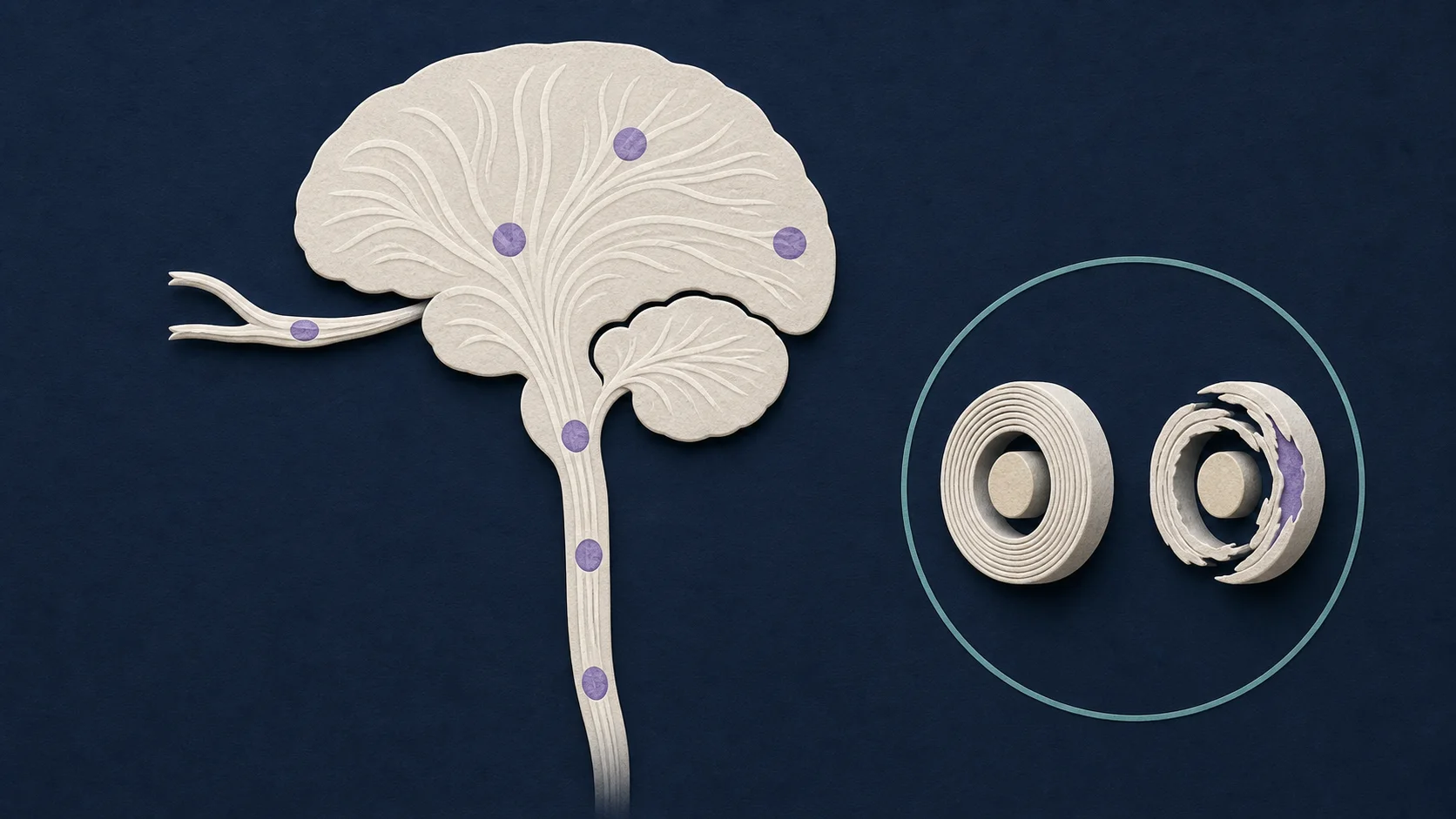
AI-generated educational schematic. Not a real medical image or an exact anatomical representation.
MS can involve the brain, optic nerves, and spinal cord; symptoms depend on the pathways affected.
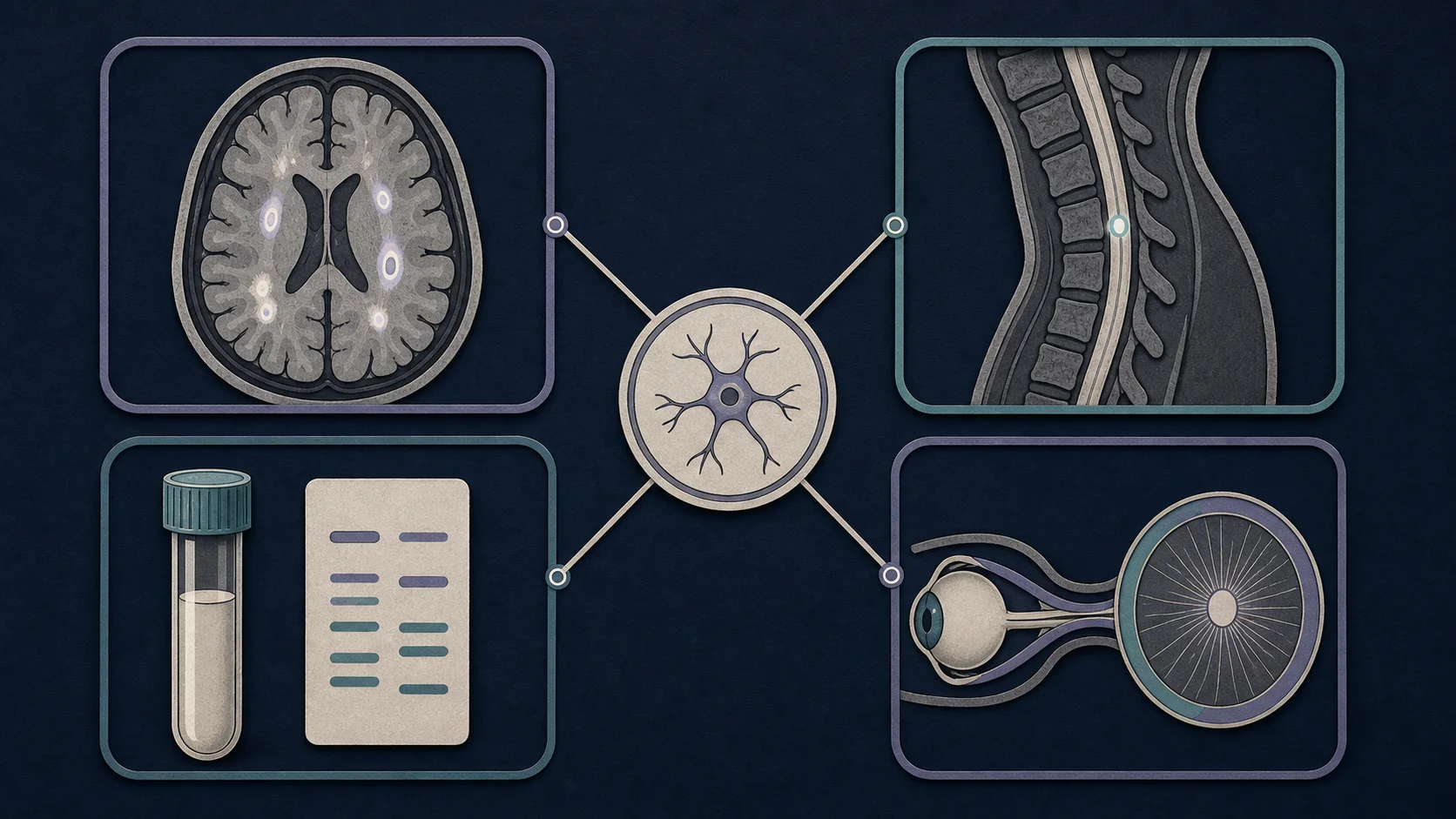
AI-generated educational schematic. Not a real medical image or an exact anatomical representation.
Diagnosis integrates a compatible presentation with MRI and selected laboratory or optic nerve evidence.
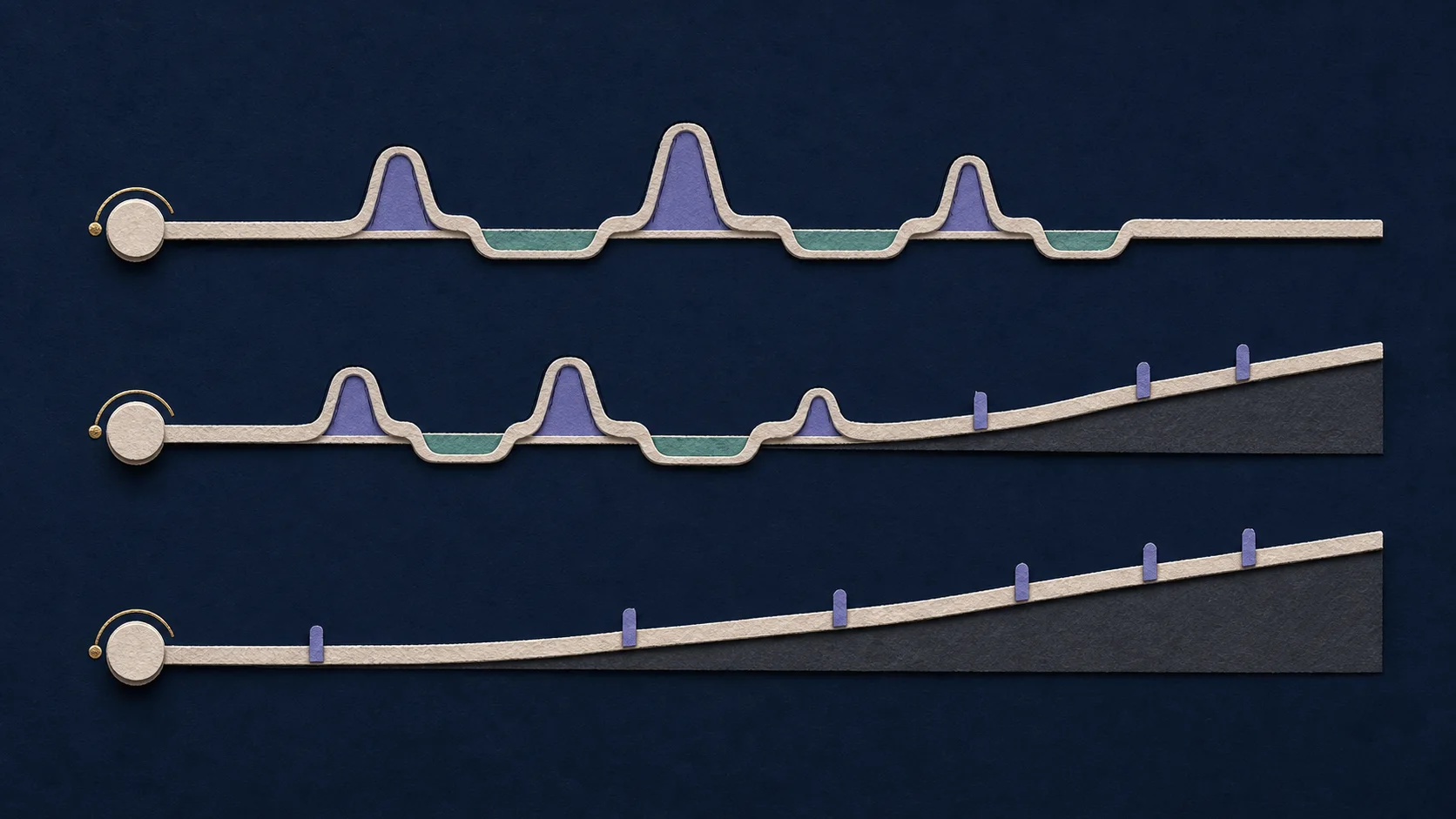
AI-generated educational schematic. Not a real medical image or an exact anatomical representation.
Course labels describe patterns over time and should be updated as activity or progression changes.

AI-generated educational schematic. Not a real medical image or an exact anatomical representation.
Long-term care combines disease modification with recovery support, symptom care, and monitoring.
A compatible central nervous system syndrome with characteristic dissemination and no better explanation.
A distinct inflammatory disorder often associated with aquaporin-4 antibodies and different treatment implications.
Can cause optic neuritis, myelitis, or brain inflammation with a phenotype and biomarker distinct from MS.
White-matter spots may be nonspecific; lesion location, shape, clinical history, and interval change matter.
Clinical context, laboratory findings, imaging pattern, and treatment response may point to another cause.
Spinal compression, nutrient deficiency, toxic injury, and inherited disorders can mimic selected MS features.
Updates how clinical, MRI, cerebrospinal fluid, optic nerve, and susceptibility-based evidence may support diagnosis in the correct context.
Read registered sourceStandardizes brain and spinal cord MRI acquisition and monitoring while emphasizing purposeful use of gadolinium.
Read registered sourceFrames starting, switching, and stopping disease-modifying therapy as shared decisions based on activity, safety, and patient factors.
Read registered sourceMS is not diagnosed from fatigue, tingling, headache, or white-matter spots alone. A specialist looks for a compatible pattern and considers whether another disease better explains the findings. [1]
Inflammation can produce an MS relapse, such as new visual, sensory, motor, brainstem, cerebellar, or spinal symptoms. Recovery may be complete or incomplete. Disability can also worsen gradually, with or without obvious relapses. Symptoms such as fatigue, pain, cognitive change, bladder dysfunction, and mood disturbance may affect daily life even when a routine examination appears stable.
The McDonald criteria organize evidence for an MS diagnosis, but they are not a self-test. MRI is central to diagnosis and monitoring. Cerebrospinal fluid, including oligoclonal bands, and objective optic nerve evidence may contribute in selected situations.
Disease-modifying therapy aims to reduce new inflammatory activity and future injury. The choice depends on disease course, current activity, prognostic features, safety, monitoring, pregnancy plans, infection risk, and individual priorities. Rehabilitation and symptom management remain important whether or not a DMT is used.
MS is heterogeneous. A useful longitudinal description records relapses, MRI activity, recovery, progression, cognition, function, treatment exposure, and competing medical or psychosocial factors rather than relying on a single course label or lesion count.