Moyamoya disease
Progressive terminal ICA-centered narrowing with characteristic collateral networks.
No single scan answers every question about moyamoya. MRI looks for brain injury, MRA maps major arteries without a catheter, DSA shows detailed collateral anatomy, and perfusion testing helps assess how well blood flow can respond when demand changes.
Diagnostic synthesis includes luminal stenosis, outer arterial diameter, collateral pathways, parenchymal injury, posterior circulation, and hemodynamic reserve. DSA remains important when anatomy is uncertain, disease is unilateral, atherosclerosis is a concern, or surgery is being planned.
AI-generated educational schematic. Not a real medical image or an exact anatomical representation.
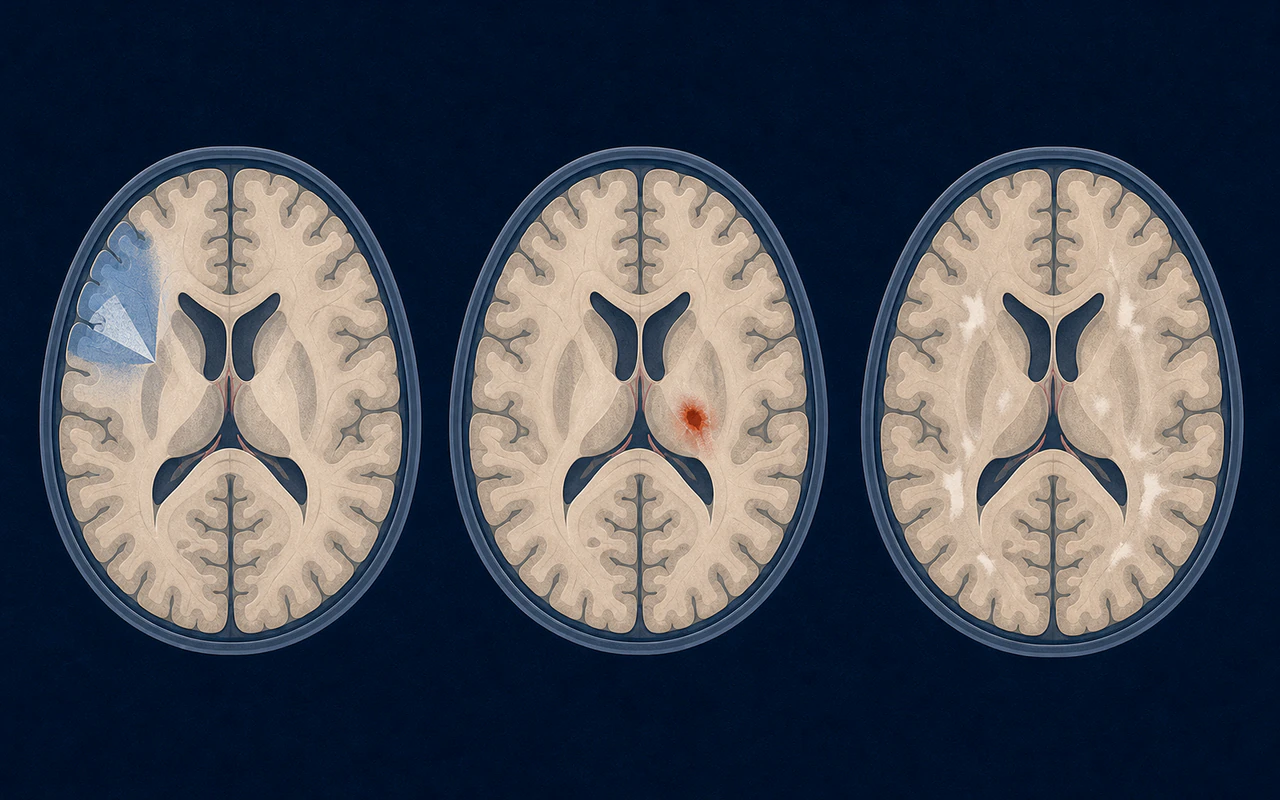
MRI evaluates acute and chronic brain injury and helps assess alternative diagnoses.
AI-generated educational schematic. Not a real medical image or an exact anatomical representation.
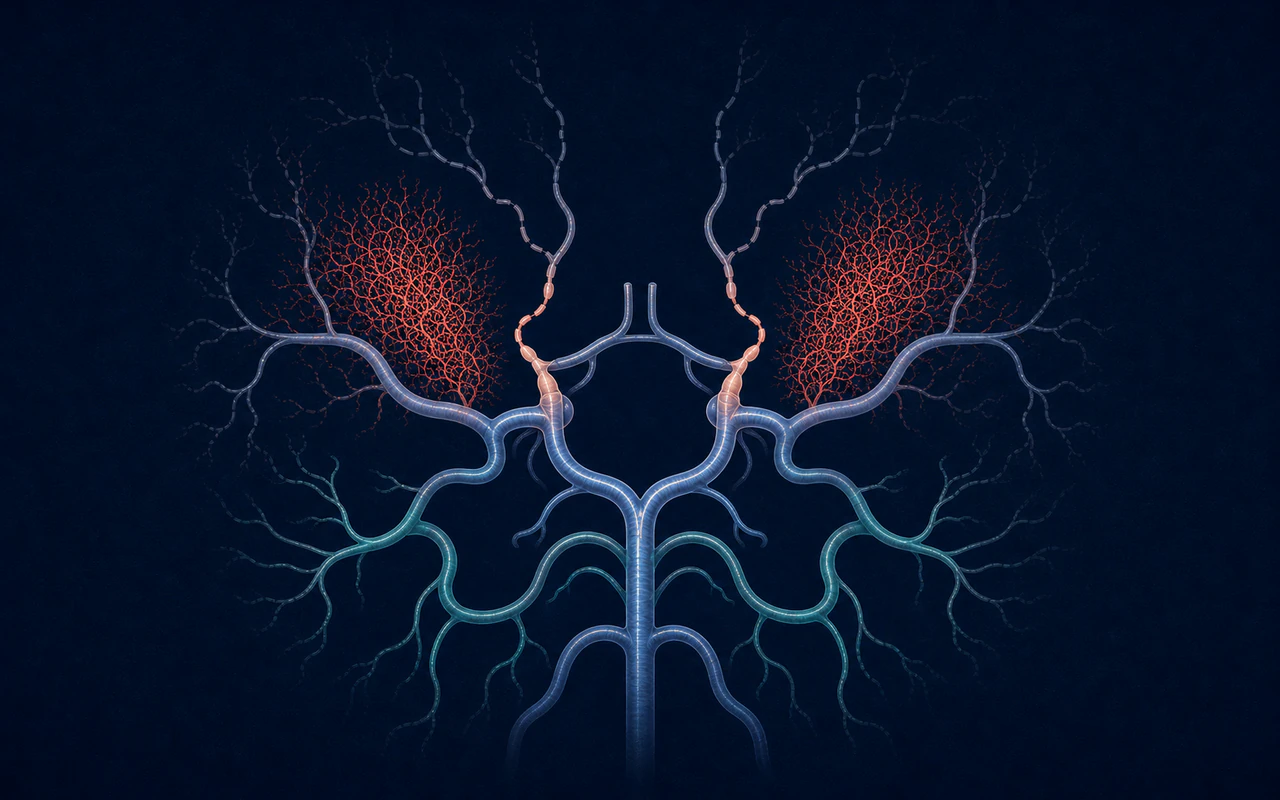
MRA provides a noninvasive view of major intracranial arterial narrowing.
AI-generated educational schematic. Not a real medical image or an exact anatomical representation.
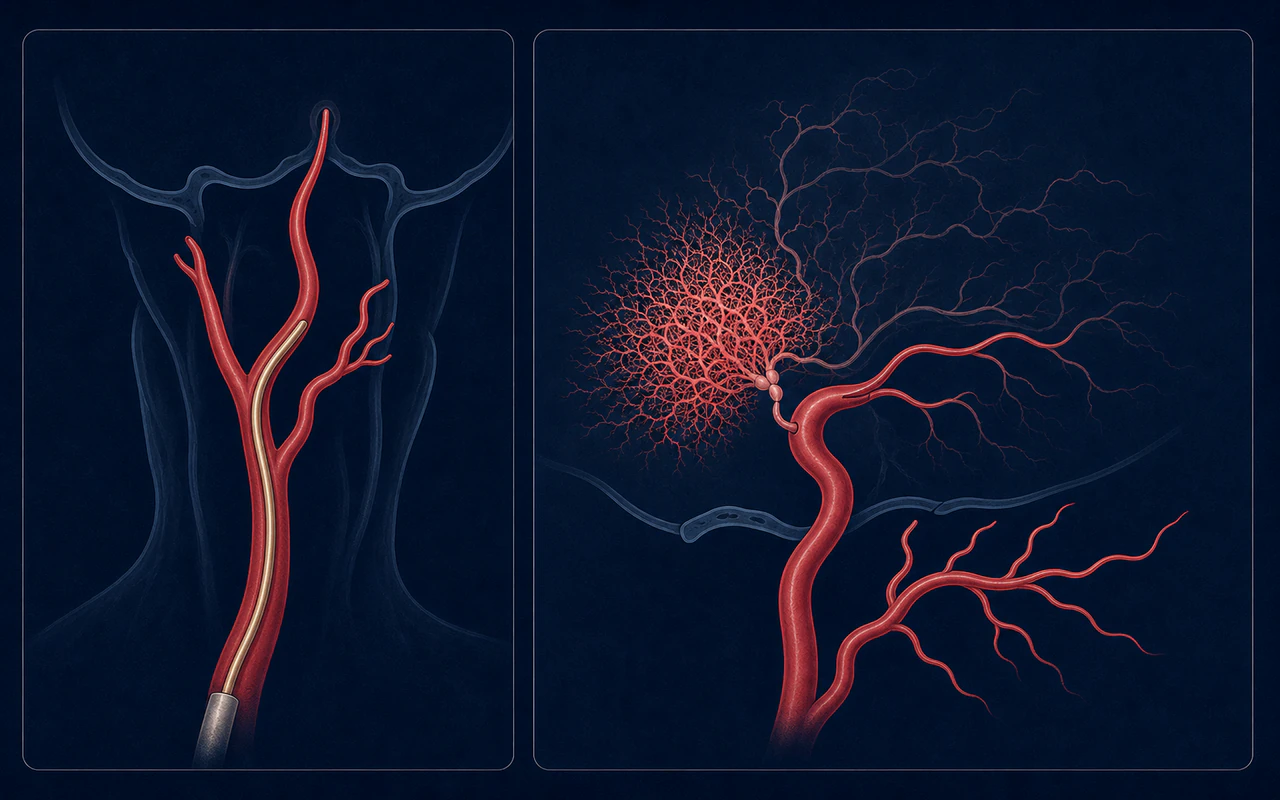
DSA defines stenosis, collateral routes, donor anatomy, and angiographic stage in high detail.
AI-generated educational schematic. Not a real medical image or an exact anatomical representation.
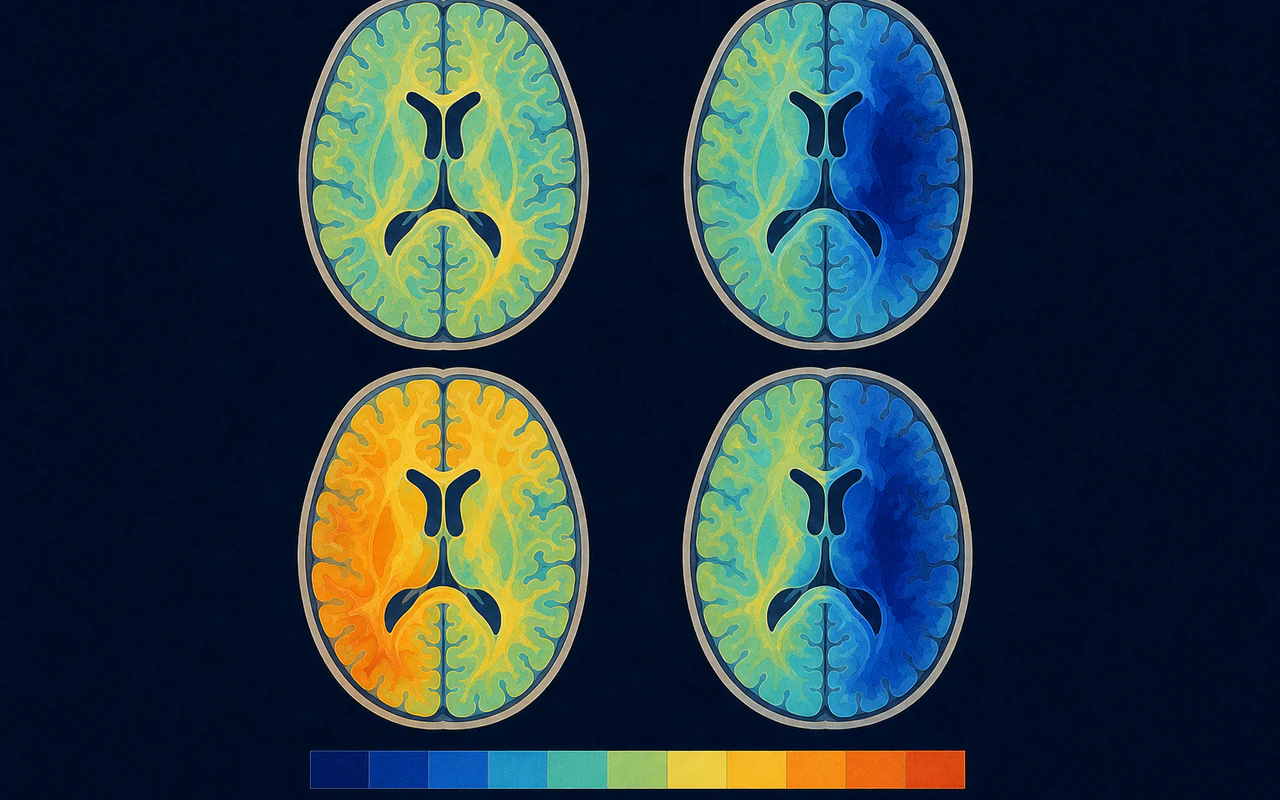
Perfusion and reserve methods assess how effectively tissue is supplied and responds to challenge.
AI-generated educational schematic. Not a real medical image or an exact anatomical representation.
Follow-up imaging may assess direct bypass patency, indirect collateral growth, perfusion, and untreated territories.
Progressive terminal ICA-centered narrowing with characteristic collateral networks.
Plaque-related stenosis interpreted with age, risk factors, vessel wall, and distribution.
Inflammatory arteriopathy assessed with clinical, laboratory, vessel-wall, and distribution clues.
Usually presents with acute headache and reversible multifocal arterial narrowing.
Arterial injury occurs in a prior radiation field and may produce a moyamoya pattern.
Focal arterial wall injury may mimic stenosis but has a different mechanism and course.
Current criteria focus on narrowing or occlusion centered on the terminal intracranial internal carotid artery and the presence of characteristic abnormal vascular networks. Both unilateral and bilateral cases can meet modern criteria. Catheter angiography is especially important when disease is unilateral, when atherosclerosis is a concern, or when anatomy is unclear. [1]
MRI looks for acute or old infarcts, hemorrhage, white-matter injury, and other diagnoses. MRA provides a noninvasive view of the major intracranial arteries. Specialized heavy T2-weighted imaging may help assess shrinkage of the outer arterial diameter, a feature used in the revised Japanese criteria.
Digital subtraction angiography, often called a cerebral angiogram, shows arterial narrowing, collateral routes, donor vessels, and external carotid circulation in high detail. It supports Suzuki staging and surgical planning, but it is invasive and requires an individualized risk discussion. [2]
Anatomic narrowing does not directly quantify how well tissue is supplied. ASL MRI, SPECT, PET, CT perfusion, and other techniques can estimate perfusion. A vasodilatory challenge may be used to assess cerebrovascular reserve. Protocols and interpretation vary, particularly because delayed collateral arrival can distort some measurements. [3]
A specialist also considers alternative causes of intracranial stenosis and whether an associated condition supports the term moyamoya syndrome. Imaging should be interpreted together: vessel lumen, vessel wall or outer diameter, collateral pattern, brain injury, posterior circulation involvement, and hemodynamics.
Suzuki stage describes a sequence of angiographic collateral patterns; it is not a linear measure of disability or current perfusion. Two hemispheres in one person may have different stages, symptoms, reserve, and treatment needs.